
Research Roulette.
“There is a dearth of robust research regarding gender affirming care” (The Cass Review, 2024). Why is that?
Republished with permission from By Jason Watson.
We will take much of our direction for this discussion from the Cass Review (2024). Dr David Bell, former staff Governor of the Tavistock Centre in the U.K. stated, “It’s important to say that the Cass Review, is the most thorough, the most wide, and most extensive review of treatment for gender distressing children ever undertaken, anywhere in the world” (Times Radio, 2024). This review (which was initiated by the British Government) describes the research into gender care as ‘remarkably weak’ and similar reviews in Finland, France, Sweden and Norway have also looked at gender research and found the studies to be weak and unreliable (Singal, 2024; Hardin, 2024). Cass goes on to state that current gender medicine research is simply not being robustly formulated and is philosophically rather than scientifically based.
Some of the reported themes that make undertaking robust research difficult especially in the last 7-10 years are.
1. Possible Legal Restrictions: Laws commonly known as Anti-Conversion laws in some countries make it a crime to attempt to change a person’s gender identity. Meaning it’s illegal to challenge, question or even remain neutral, regarding a client’s identified gender if the purpose is to change their gender identity. Professionals are worried about falling foul of the law & their workplace guidelines. Worried about the consequences if the research they are undertaking seems to challenge a client’s perceived identity. Transgender Health (TGH) appears to be the only health field where this is the case. Please note: A ‘Watchful Waiting’ neutral response does not appear to be at odds with NZ’s Anti-Conversion law (Goulter & Penk, 2024).
2. Transgender Health Leadership: When Cass discovered the poor quality of research in this field she along with the University of York contacted the TGH services in the UK asking for their full involvement in running some robust research in their clinical spaces. Every facility in the U.K. except one refused to be involved in this research initiative (Cass, 2024).
3. Hitting the Glass Journal Ceiling: Gregory, Davis and Sample, (2024) spoke of the challenge of getting studies published in high-profile journals. They raised concerns that some journal editors may prefer to reject research that questions or is critical of current practices regarding Gender Affirming Care rather than face potential criticism or cancelling. Consequently, research that flags knowledge gaps in TGH can become ‘ghettoised’ (emphasis by Devlin & Sample, 2024) into journals with less profile.
4. Hate-speech accusations: Claiming that researchers whose research demonstrates outcomes that are perceived as a challenge to the pro Gender Affirming Care pathway are transphobic, hateful, harmful and misguided (Bridges, Khaira 2022).
5. Fear of Cancellation: That this may lead to the researcher, academic or practitioner working on ‘the ground floor’ being bullied in the workplace at the least, or professionally cancelled at the most (Favaro, 2022; Siddique, 2022; Spencer-Lane, 2024; Lexology, 2024; First do no harm, 2024; UKCP, 2024; Ely, 2024;Somerville, 2022; Lindsay, 2023; Dixon, 2022; Canvin et al, 2022). This fear makes it harder to undertake robust research regarding the efficacy of TGH procedures. Cass when interviewed after the release of the Cass review stated she now feels worried about her physical safety out in public (Beal, 2024), many others who suggest another narrative have said similar things (Pietzke, 2024).
6. Lack of discussion or debate: Open debate is a cornerstone of clinical critique. However even experienced clinicians, researchers and academics are increasingly scared to openly discuss their views on the treatment of gender-questioning children or youths (Devlin & Sample, 2024; Baxendale, 2024; Pietzke, 2024).
7. Difficulty with change: Change is seen and is needed in all areas of healthcare. Feeling they are able to change their practice allows academics to pay attention to objective systematic reviews regarding TGH care. And to the definable potential benefits as well as harms and outcome uncertainties for these vulnerable children and youth (Abbruzzese, Levine, & Mason, 2023). However, changes that do not sit well with the current client led narrative are slow and reluctantly undertaken.
8. Skewing the playing field: The highest form of researched evidence is a Meta-Analysis or Systematic Review (University of Canberra, 2024). With academics fearful of making research to clarify or fill any knowledge gaps, many systematic reviews will be simply comparing like with like and will not look at a variety of data. It appears this is being done purposefully as some individuals and groups did not believe the results of a thorough Meta-Analysis would paint this field in a favourable light. This clinical research environment that currently exists has a dearth of robust data and therefore I am critical of any clinical practice founded on this research.
9. Manipulation of TGH research. The researchers for the Cass Review (2024) examined the veracity of 103 research articles on gender affirming practices. With the help of the University of York they found the vast majority of the 23 clinical guidelines that were reviewed were not evidence based or independent. The Cass team also stated that with one meta-analysis paper researching puberty blockers they found that only one study was of high quality (one out of fifty). Also, in another meta-analysis on the use of hormone treatment, only one study was of sufficiently high quality (one out of fifty-three) with little or only inconsistent evidence on key outcomes. Most of these research papers lacked an evidence-based and independent approach and they lacked information about how the recommendations were developed (Gregory, Davis & Sample, 2024). This quality of TGH research data currently appears to be the norm.
Here is one example of this manipulation of TGH research. We will look at one paper from the New England Journal of Medicine (which is the most widely read, cited, and influential general medical periodical in the world). Most of the investigating regarding this study was undertaken by Jesse Singal (Singal, 2022; 2024). This NEJM study is a National Institution of Health funded study, looking at outcomes in four youth gender clinics. The 2023 article’s lead author is Dr Diane Chen, and was titled, Gender-Affirming Hormones Improve Mental Health in Transgender and Nonbinary Youth.
This was a study of 315 young people aged from 12-20 years, which is a small-medium sample size. The age limit for entry was reduced down to start at eight years old but no children this young were admitted to the study. All children and youth were given a $100 gift card for their involvement. The study when it was published emphatically states that cross sex and puberty blocking hormones were beneficial to youth mental health. One of the headlines from the study by Dr Robert Garofalo, one of the principal investigators for the study reads, “Our results provide a strong scientific basis that gender-affirming care is crucial for the psychological well-being of our patients.” The children and youth were receiving other psychological therapy during this time and the researchers tout a two-year increase of 0.82 points on a 100-point Positive Affect scale as evidence that hormones work with these children and youth.
The authors published the study protocol (outline of study shape) before the main body of the study (Chen, 2019). This included the choosing of eight different variables of youth trans mental health. These children and youth in the study were to be put on cross sex hormones or puberty blocking hormones. The research hypothesised that if these hormones were beneficial, then one or more of these eight variables will be seen to have improved. If you compare the published study (Chen, 2023) to the protocol document (Chen, 2019), you’ll notice that of the eight key variables the researchers were most interested in depression, anxiety, gender dysphoria, trauma symptoms, self-injury, suicidality, body esteem, and quality of life” only depression and anxiety are reported in the NEJM paper. That’s two out of eight, or 25% of the variables covered by the researchers’ hypothesis in their protocol document. See also Chen, (2020). The authors do include these remaining two variables and add other variables not included in the original study protocol when they ‘write up’ their study.
Points to Ponder or Wonder about:
The study showed that the anxiety and depression variables moved in a positive direction for trans boys (natal females) but not trans girls (natal males). Could this simply be the result of experiencing Testosterone?
The researchers’ hypothesis changes in the NEJM study. In the 2019 protocol it reads, “Patients treated with gender-affirming hormones will exhibit decreased symptoms of anxiety and depression, gender dysphoria, self-injury, trauma symptoms, and suicidality and increase [sic] body esteem and quality of life over time.”
However… In the 2023 study it reads, “We hypothesized that [after these kids were administered hormones], appearance congruence (new), positive affect (new), and life satisfaction (new) would increase and that depression and anxiety symptoms would decrease (Affected by Testosterone?). They also hypothesized that improvements would be secondary to treatment for gender dysphoria, such that increasing appearance congruence (new) would be associated with concurrent improvements in psychosocial outcomes.” There was no mention of suicidality, and self-injury. Why?
“Gender dysphoria” is briefly mentioned in the study, but there’s no mention at all of any gender dysphoria scale with which to measure it, however several other scales for all other variables were mentioned. In the supplementary materials (Chen, 2019; Chen, 2023a) they do mention the use of two GD scales (the Transgender Congruence Scale and the Gender Minority Stress and Resilience Scale) reportedly not to measure GD however, as their protocol document explains, but because they thought they were bad tools and wanted to demonstrate this. This rationale sounds very odd!
The 2019 protocol document includes a “Letter of Amendment” removing these tools. They still use both tools at the 2 year follow up visit however, but no mention of results was made in the paper. Again this rationale does not make sense. Perhaps the results found by using these tools did not appeal to their expected outcomes?
However the authors did make mention of the one Transgender Congruence Scale subscale in the study (not the whole of the data, just one subscale). And according to the 2019 protocol, the kids in this cohort were also asked about their DSM-5 gender dysphoria symptoms until a separate Letter of Amendment(2021) halted the asking of these questions. Why was data collected, then not collected and only partly referenced in the final study? Is this cherry picking?
The phrase “quality of life” and any mention of the Health-Related Quality of Life Scale do not appear in the paper. Quality of life and life satisfaction (new variable) are not the same construct as they’re listed under two different variables in the study protocol. Why the change, what data was collected and using what tool?
The authors mention two completed suicides (one after six months and one after one year), and mention “suicidality” but there’s zero mention of a suicidality scale (similar to the Gender Dysmorphia missing scale). It is hugely conspicuous by its absence. The authors mention eleven instances of ‘suicidal ideation’, but again no mention about the suicidality assessment tools used. The authors definitely have data on body esteem and suicidality because they report the baseline numbers for these variables in another study (Chen et al, 2020). Why don’t they provide more data here, or publish it in the Supplementary Index?
Regarding completed suicides, the closest we can get for an annual estimate for the general population within the age range of the study (12–20) is 14.2 suicides per 100,000 members of the 15–24 age band. This points to the suicide rate of these children/youth being ‘significantly higher’ than the general population.Why is this?
The other variables not mentioned in the study, also go missing in the appendix (Chen, 2023a). If the authors wanted to explain the absence of certain variables without taking up potentially limited space in the paper itself, this would have been a good place to do so. Why don’t they? They seem to have picked plenty of cherries!
The researchers are crystal clear about the original variables they are most interested in, in the protocol document that supposedly underpins this study. Then when they publish the paper their hypothesis is substantially different, and they present their interest in appearance congruence in the hypothesis as if they had done so all along, when there’s no evidence that was the case.
In the first paragraph of the study the importance of appearance congruence is underlined, however the phrase appearance congruence doesn’t get mentioned once in the protocol document.
The study states that “there were significant within-participant changes over time for all psychosocial outcomes in hypothesized directions.” However they did not report at all on six of eight of the variables tested for, and added into the study other variables without explanation. Why would that be?
The researchers are touting a two-year increase of 0.82 points on a 100-point Positive Affect scale as evidence that hormones work with these youth. Is this positive change solely due to hormone therapy?
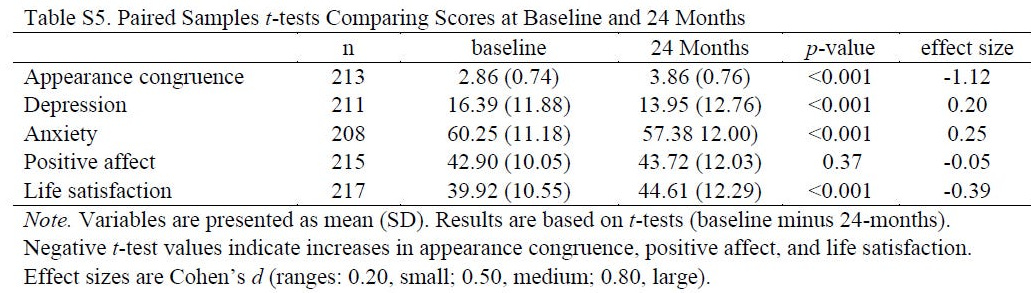
It’s impossible to attribute the small improvements observed in this study to hormones rather than to the other forms of therapeutic treatment that took place at these clinics.
So is this an example of what Cass describes as dissapointingly poor research which is philisophically rather than scientifically based. Have a look yourself and see what you can see!
References:
Abbruzzese, E., Levine, S. B., & Mason, J. W. (2023). The Myth of “Reliable Research” in Pediatric Gender Medicine: A critical evaluation of the Dutch Studies—and research that has followed. Journal of Sex & Marital Therapy, 49(6), 673–699. https://doi.org/10.1080/0092623X.2022.2150346
Baxendale, S. (2024). The impact of suppressing puberty on neuropsychological function: A review. Acta Paediatrica, Vol 113(6), 1156-1167.
Beal, J. (2024). Hilary Cass: I can’t travel on public transport after gender report. (as of 16/6/2024.
Bridges, K. (2022). Professor from Berkeley School of Law. Speaking to Senator Josh Hawley in a Senate Judiciary Committee, 13th July 2022.
Canvin, L., Twist, J., & Solomons, W. (2022). ”I don’t want to say the wrong thing”: mental health professionals’ narratives of feeling inadequately skilled when working with gender diverse adults. Psychology & Sexuality, 14(2), 337–350. https://doi.org/10.1080/19419899.2022.2118070
Cass Review. (2024). Final Report: Cass Review. https://cass.independent-review.uk/home/publications/final-report/; 15th May 2024.
Chen, D. (2019). Study Protocol. Study: Gender-Affirming Hormones Improve Mental Health in Transgender and Nonbinary Youth. https://drive.google.com/file/d/16lYGytKbKV_aakil7kucl1UhkGlovPLO/edit
Chen D, Abrams M, Clark L, Ehrensaft D, Tishelman AC, Chan YM, Garofalo R, Olson-Kennedy J, Rosenthal SM, Hidalgo MA. (2020). Psychosocial Characteristics of Transgender Youth Seeking Gender-Affirming Medical Treatment: Baseline Findings From the Trans Youth Care Study. (2020). J Adolesc Health. 2021 Jun;68(6):1104-1111. doi: 10.1016/j.jadohealth.2020.07.033. Epub 2020 Aug 21. PMID: 32839079; PMCID: PMC7897328.
Chen, D. (2023). Study: Gender-Affirming Hormones Improve Mental Health in Transgender and Nonbinary Youth. January 18, 2023; https://www.luriechildrens.org/en/news-stories/study-gender-affirming-hormones-improve-mental-health-in-transgender-and-nonbinary-youth/
Chen, D. (2023a). Supplementary Appendix. Gender-Affirming Hormones Improve Mental Health in Transgender and Nonbinary Youth. https://drive.google.com/drive/folders/19cECwGjXDMRK2JITzmMnxbYHDl5H5l56
Dixon, H. (2022). Nurses ‘sacked for speaking out about transgender patients on single-sex wards’. 10th Feb, 2022. https://www.telegraph.co.uk/politics/2022/02/10/nurses-sacked-speaking-transgender-patients-single-sex-wards/
Devlin, H., and Sample, I. (2024). ‘This isn’t how good scientific debate happens’: academics on culture of fear in gender medicine research. The Guardian. https://www.theguardian.com/society/2024/apr/12/this-isnt-how-good-scientific-debate-happens-academics-on-culture-of-fear-in-gender-medicine-research
Ely, J. (2024). Nurses and midwives may face being struck off for intentionally mis-gendering patients under updated guidance that claims it’s a ‘BELIEF’ that people can’t swap sex.
Favaro, L. (2022). Researchers are wounded in academia’s gender wars. Sept, 15th 2022. https://www.timeshighereducation.com/depth/researchers-are-wounded-academias-gender-wars
First do no harm, (2024). James Esses reaches settlement with UK Council For Psychotherapy. 20th June, 2024.
Gregory, A., Davis, N., and Sample, I. (2024). Gender medicine ‘built on shaky foundations’, Cass review finds. Analysis finds most research underpinning clinical guidelines, hormone treatments and puberty blockers to be low quality. The Guardian. https://www.theguardian.com/society/2024/apr/10/gender-medicine-built-on-shaky-foundations-cass-review-finds
Goulter, G., and Penk, A. (2024). Students and Social Transition A gender identity policy guide for New Zealand schools. https://assets-global.website-files.com/6585003e5fe6d5aea67f0003/6638248287bd3700e18c3891_Students%20and%20Social%20Transition%20-%20A%20gender%20identity%20policy%20guide%20for%20New%20Zealand%20schools.pdf
Hardin, N. (2024). Psychologist Dr. James Cantor details harms of ‘Transitioning’ Kids. Alliance Defending Freedom. https://adflegal.org/article/psychologist-dr-james-cantor-details-harms-transitioning-kids
Lindsay, B. (2023). · Nurse tells B.C. hearing she’s not transphobic, but calls gender identity ‘metaphysical nonsense’. CBC News · Posted: Nov 03, 2023. https://www.cbc.ca/news/canada/british-columbia/bc-amy-hamm-disciplinary-hearing-nov-3-1.7018573
Lexology, (2024). Joanna Phoenix v Open University (2024). Lexology.com;
Pietzke, T. (2024). The Unlikely Whistleblower with Tamara Pietzke | Episode 161.
Gender, A wider lens. Apr 26, 2024.
Spencer-Lane, T. (2024). Why social worker won harassment claims against council and regulator over gender critical beliefs. 17th Jan 2024. Community Care UK.
Siddique, H. (2022). Maya Forstater was discriminated against over gender-critical beliefs, tribunal rules. Researcher lost job at thinktank after tweeting that transgender women could not change their biological sex. 6th July 2022. The Guardian. Singal, J. (2023). On Scientific Transparency, Researcher Degrees Of Freedom, And That NEJM Study On Youth Gender Medicine (Updated). Singal-Minded. Jan 31st 2023.
Singal-Minded On Scientific Transparency, Research Degrees of Freedom,And That NEJM Study OnYouth gender Medicine (Updated)
Somerville, E. (2022). Nurses boycott Royal College after chief rejects gender-critical views. The Telegraph. 3rd June 2022. https://www.telegraph.co.uk/news/2022/06/03/nurses-boycott-royal-college-chief-rejects-gender-critical-smears/
Singal, J. (2022). “Science Vs” Cited Seven Studies To Argue There’s No Controversy About Giving Puberty Blockers And Hormones To Trans Youth. Let’s Read Them. Jun 10, 2022
Singal, J. (2024). The End of Transgender Care for Minors? The Dispatch Podcast. Apr 26, 2024. https://gimletmedia.com/shows/science-vs
Times Radio, (2024). Puberty blockers have ‘seriously damaged generations of children’ Tavistock whistleblower. Times Radio, 10th April 2024.
University of Canberra, (2024). The Evidence Hierarchy: What is the “Best Evidence”? On 20th June 2024. https://canberra.libguides.com/c.php?g=599346&p=4149721
UKCP, (2024). UKCP guidance regarding gender critical views. 20th June 2024.

Here is some background on 'research roulette.' The first data ever collected on LGBT children came from MA which became an enclave for the cult's agenda. It was called the MA Youth Risk Behavior Survey and was done in 1995. Robert Garofalo, mentioned in this post and the lead the arm of transitioning children at Lurie, was among researchers. Among the info asked is sexual orientation and gender identity (SOGI). Does anything SOGI belong near children? The interest in the data is to make more data and grow a population. From there grows industry. The entire thing is a sham.
MA continues to do this study. There is a national one now done by the CDC and yes, it contains SOGI data since 2023. Once they collect data, even if it is based on a bogus concept like gender identity, they have captured a patient population.
You can read about another early and important study to industry here dubbed "Hatred in the Hallways." It basically accuses US schools as being 'hateful' toward LGBT based on little data and bogus concepts that do not belong near children. It is about markets. https://margox.substack.com/p/traumatizing-american-families?r=1kuq0
Thanks for an excellent critique of yet another study ‘proving’ GAC is effective. It’s all so sickening—ruining the lives of a legion of young people under the banner of medical science. Sickening too that such studies are reviewed positively by peers and published in ‘reputable’ journals. Sorry, but on behalf of so many broken young people and grief-stricken families: may all involved rot in hell.