
What is the view from the top?
A brief investigation of one of the most well renown child and adolescent gender clinicians in the world.

According to ChatGPT in January 2026 the most well-known transgender child and adolescent doctor in the world is Dr Johanna Olson-Kennedy (JOK). She is board certified as a pediatrician since 2001 and adolescent medicine physician since 2003. She was the Medical Director of the Center for Trans youth Health and Development at Children’s Hospital Los Angeles which was the largest such centre in the USA. She is also a principal investigator on major NIH (American Ministry of Health) funded studies of puberty blockers and gender-affirming care in youth, she is one of the most frequently referenced clinicians in debates over pediatric gender medicine and regularly appears in medical, legal, and policy discussions worldwide. She also on multiple occasions has provided expert opinion in court cases within the USA.
Over her nearly twenty-year career she has treated a significant number of trans youth. She estimates prescribing ‘gender-affirming hormones’ to over 1,000 children and youths. She is a long-standing member of the World Professional Association for Transgender Health (WPATH), joining in 2010, and has held leadership roles in its regional affiliate, the U.S. Professional Association for Transgender Health (USPATH). She was appointed to the Executive Board of (USPATH) in 2022 and is currently the president-elect of the USPATH.[13] She has authored 20 plus peer-reviewed research articles and about 30 others works such as chapters in books or editorials. On the surface of things, she seems to be a credible expert in her chosen field. What if we look a little deeper however?
In about 2016 JOK received from the NIH a multi-million-dollar grant to create and run a research study. The study started soon after and concluded in about 2018/2019 and by the end of the study the cost was nearly 10 Million Dollars. The study was described as “by far the largest such project in America”. She became lead author in the study looking at the benefits of gender affirming care (initiated with Puberty Blockers) on the mental and emotional health of trans youth. She was not pleased with the results of the study however and delayed publishing it for nine years until she was forced to (20, 21). How do we know this? The hiding of the research was discovered by the New York Post. When asked why she had hidden this study by the New York Post, she replied she ‘delayed publication of some of her results because of fears that they would be weaponized in a heated political climate’.
An example of what she was hoping to avoid was authored soon after the New York Post article by author J.K. Rowling. She wrote this in response to the NY Posts article on JOK’s hidden research, that “…We must not publish a study that says we’re harming children because people who say we’re harming children will use the study as evidence that we’re harming children, which might make it difficult for us to continue harming children!” 22. Now politicians are asking to see the results the NIH paid to have her research and are asking why she has hidden the results for so long. Republican senators published an open letter addressed to the director of the NIH which requested further information about this project and reiterated the importance of transparency in medical research that the NIH supports with public funds.[18]
This was not a good look for JOK! So how does the academic world view the credibility of research created by JOK? On the surface she is still generally seen as an expert in her field with good standing with her peers. Bearing this in mind however this question, how usable and accurate is the research she has authored or co-authored? For the answer to this question, we will look to the GRADE research rating tool. The GRADE or (Grading of Recommendations Assessment, Development and Evaluation) approach is the most widely accepted, internationally recognized framework for evaluating the quality of evidence and strengthening recommendations in healthcare. They rate research study results in four levels of certainty and generalizability. The higher the rating, the more certain the evidence is and more able to be used in clinical settings. The highest rated research would use Randomised Controlled trials, with outcomes proven to be repeatable in different settings. The lowest rated studies such as observational studies create research questions or theories that need more robust research in order to be safely and effectively used in clinical practice.
The GRADE levels of research certainty/validity are...
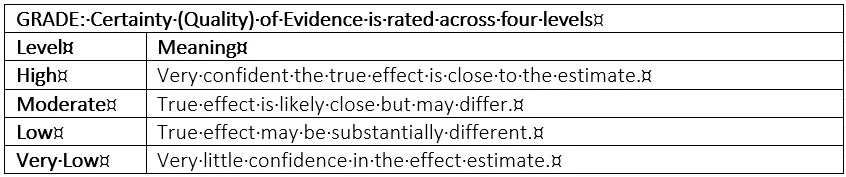
1. High: With these studies you can be very confident that the true effect is close to the estimate. These studies typically start with randomized controlled trials.
2. Moderate: With these studies you can be moderately confident; the true effect is likely close but may differ substantially. These difference(s) may result from some limitations in study quality or consistency. Examples of these limitations might be for concerns regarding bias risk or small sample size.
3. Low: With these studies you can have limited confidence in the reliability of his evidence and the true effect may be substantially different from the estimate. Examples of these studies are observational studies. These studies are inherently more vulnerable to bias and confounding than randomized controlled trials (RCTs) therefore we should be cautious about how confidently we interpret and generalise their findings.
4. Very Low: With these studies you can have very little confidence; the true effect is likely substantially different. Evidence may be downgraded due to bias, imprecision, inconsistency, or indirectness.
So, let’s have a look at JOK’s Grades! I googled research articles she has been lead author or co-author in from 2011 onward. With JOK’s articles 1, 2, 3, 4, 5, 6 the evidence quality was deemed “Very Low”. Her best research outcomes I found were these articles 7 and 8 and the outcomes were rated Low to Very Low. Lastly there is the above mentioned 2019-2025 hidden study (9) on Mental and emotional health of youth after 24 months of gender-affirming medical care initiated with pubertal suppression. The certainty of evidence was also assessed as Low to Very Low. Dr Hilary Cass author of the 2024 Cass Review stated that there is a dearth of robust research regarding gender-affirming care, that the research is of disappointingly poor quality, built on shaky ground and ideologically rather than scientifically based. It looks like this claim is true for these studies we have examined from JOK.
Here is her 2019 study in more detail. The GRADE assessment found that the…
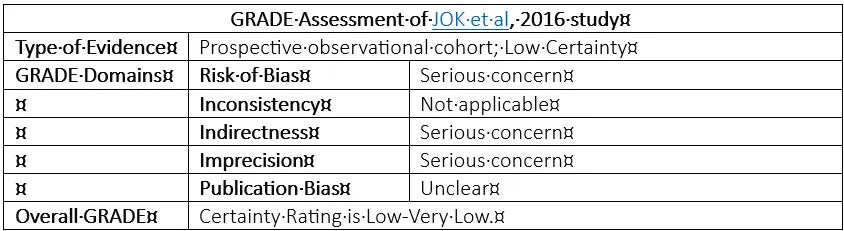
1. Risk of Bias. Was of Serious Concern
2. Inconsistency. Concerns not applicable
3. Indirectness. Was of Serious Concern
4. Imprecision. Was of Serious Concern
5. Publication Bias. Unclear if any Concern
6. The overall Grade assessment. Certainty rating for this research was Low-Very Low/
What about the WPATH association which JOK is a member of, and the USPATH which she is president of? I found the three most referenced WPATH studies and looked at how they stack up with the GRADE assessment tool? One of these studies was the 2011 ground-breaking research now known as the Dutch Protocol. It investigated puberty suppression in adolescents with gender identity disorder. The certainty of this evidence was rated as Very Low. In 2017 again, the creators of the Dutch Protocol published a guideline on Endocrine treatment of gender-dysphoric/gender-incongruent persons based on its 2011 study. This was widely referenced by WPATH. The evidence underlying the guidelines were rated as Low to Very Low. And lastly WPATHS own Standards of Care 8th Edition (SOC8) frequently references this Turban et al 2020 study on pubertal suppression for transgender youth and risk of suicidal ideation. The GRADE assessment tool states the certainty in the evidence here is Very Low.
The score card of transgender research does seem to ring true to Dr Cass’ assessment of it. The main reason research in this field has such poor reliability in its evidence is the researchers exclusively fail to use a control group. Therefore, they cannot compare the outcome of treatments between groups. Until this is done the evidence from this research will continue to scientifically be of low value and reliability. And also, as seen from JOK’s 2019 study, evidence that does not fit within the authors pro-trans view of the world is simply not published.
What about the publicly available views and quotes of Johanna Olson-Kennedy?
Is all of this evidence a ‘hatchet job’ just made up by others to discredit JOK? What does she say herself? JOK has been quoted in press (also on youtube) as saying that if a young person who has had a double mastectomy (removal of breasts) later decided they wanted breasts again, they could just “go and get them” (i.e., get breast implants or reconstructive surgery).
In the Gender GP webpage JOK states regarding a professionals role in caring for transgendered people that “I think that living with uncertainty is okay. I think we need to drop our pursuit of certainty and work on our pursuit of compassion”. She also told ABC News that “We often ask parents, would you rather have a dead son than a live daughter? This narrative is used to pressure parents into allowing gender ‘treatments’ for their children. She also states that, “this idea that we’re gonna support people at a young age is very, very new.“ JOK believes that the earlier in life kids make the social transition, which means living in the world as the gender they feel they are, the better these at-risk children function. Gender identity isn’t a choice; it’s set at birth. Kids know whether they’re a boy or a girl on the inside by the age of three or four she told ABC News.
What about the once trans always trans view? JOK stated, “If it’s okay at 13 but their understanding of gender changes when they get older it's not going to be the right thing for them anymore and they’ll navigate that.” … “… you should talk about it when you're three, when you’re 15, when you’re 21, it's absurd, we really have to understand that people know their gender – they're not making a decision about their gender, they’re making a decision about what to do with it if it doesn’t match their assigned sex at birth.” She makes the unevidenced claim that underlying mental health diagnoses are not the cause of gender dysphoria, although it’s not clear how to prove or disprove this if we don’t explore these issues in connection with the gender dysphoria.
Also, she explains her view of gender to children this way. At the 2017 USPATH conference she tells her peers that she asks kids, “do you ever eat Pop Tarts?” And the kid was like, oh, of course. And I said, “well, you know how they come in that foil packet?” Yes. “Well, what if there was a strawberry PopTart in a foil packet, in a box that said ‘Cinnamon Pop Tarts.’? Is it a strawberry Pop Tart, or a cinnamon Pop Tart?” This is the rationale, a totally unproven rationale that the most prominent child and adolescent transgender doctor in the world uses to convince children that they are agender that is in the wrong body. Lastly she does recognize that hormone therapy produces some bodily changes that are permanent (e.g., voice and chest changes) and others that are reversible, but states that hormone use is safe and effective. However, there is significant evidence which states the use of hormones can be very harmful. (25, 50, 51, 52, 53, 58, 59, 60). In fairness as these studies were also not randomised controlled trials the evidence was ‘GRADED’ as low to very low certainty for generalisability.
How can this be legal, you might ask? There is no simple answer to this question. What is clear that after the hiding of the 2019 study for nine years, the release of the Cass Review in 2024 and the American NIH version in 2025, the Center for Trans youth Health and Development at Children’s Hospital Los Angeles has been closed and JOK’s role there has ended. In 2024 JOK was sued by a detransitioner—for medical negligence after overseeing the mentally ill girl’s gender-transition starting at 12 and double mastectomy at 14. The plaintiff reports having suffered from severe, worsening mental illness while JOK oversaw her gender-transition treatment, including her mastectomy. The case was dismissed as the ‘statute of limitations’ for medical malpractice (three years) had passed. The plaintiff Clementine Breen has appealed this decision to a higher court.
So, this is an overview of Dr Johanna Olson Kennedy in respect of her views and practice in the field of children and adolescents with gender dysphoria. I’m sure that this overview misses parts, but the overview creates a general picture of arguably the most prominent pediatric gender clinician in the world. I think this is pretty scary, what about you?
For more on this author.
I wish just ONE of mainstream media would publish this article. But they won't. Because if they did that would essentially be admitting that they, like JOK, are complicit in intentionally harming children & fragile young people. I'm praying for the day this atrocity gets exposed for the crime that it is.
I think she should be rotting in a jail cell for serial child abuse on a mass scale.